Free Medication Administration Record Sheet Form
Things You Should Know About This Form
What is a Medication Administration Record Sheet?
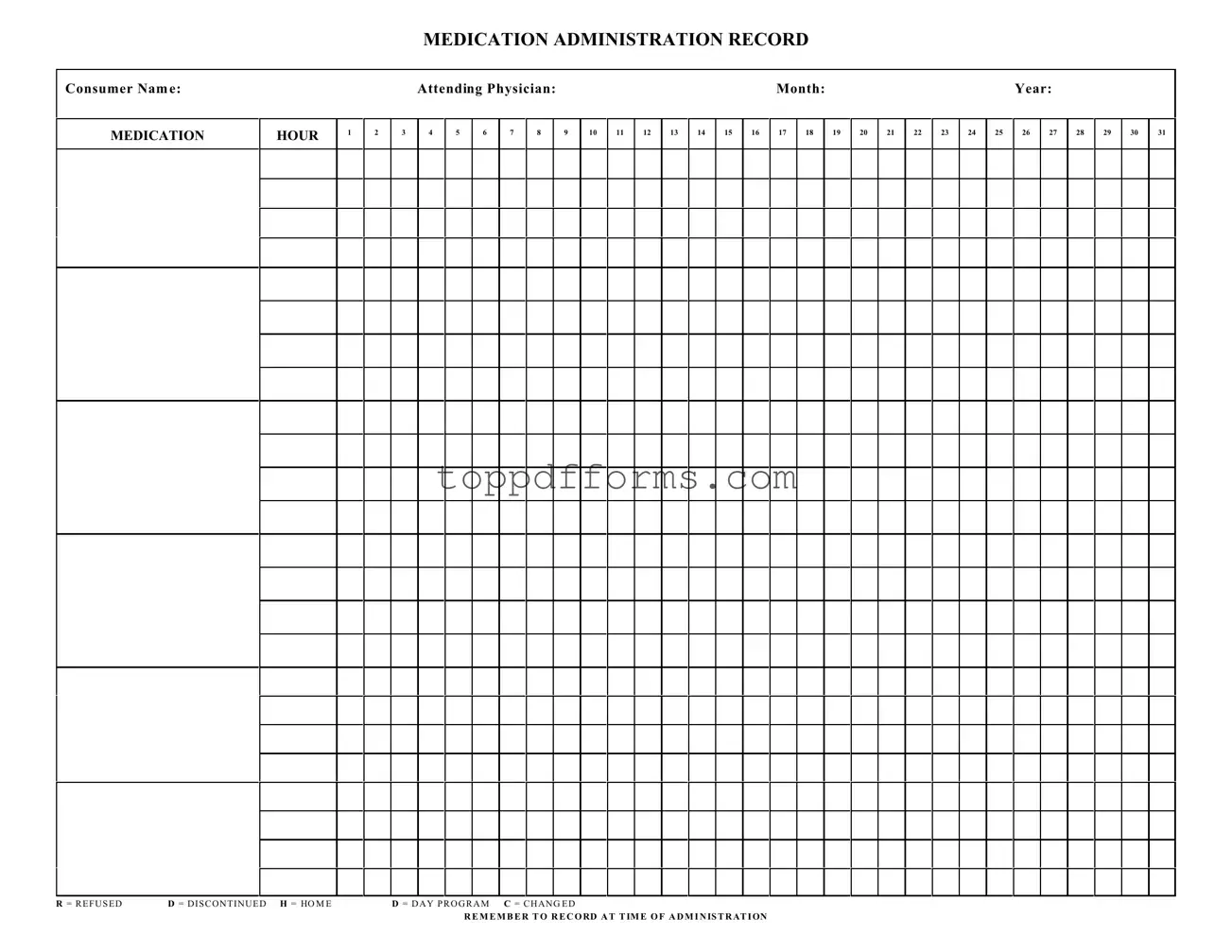
The Medication Administration Record Sheet is a form used to track the administration of medications to individuals. It helps caregivers document when and how medications are given. This ensures that patients receive their medications on time and as prescribed.
Who should use the Medication Administration Record Sheet?
This form is primarily used by healthcare providers, caregivers, and staff in residential facilities or day programs. Anyone responsible for administering medications should utilize this sheet to maintain accurate records.
How do I fill out the Medication Administration Record Sheet?
Start by entering the consumer's name, the attending physician's name, and the month and year at the top of the form. Then, for each medication, record the time of administration in the appropriate hour column. If a medication is refused, discontinued, or changed, mark it clearly using the designated letters (R, D, H, C) provided on the form.
Why is it important to record the time of administration?
Recording the time of administration is crucial for ensuring that medications are given at the correct intervals. This helps prevent missed doses and ensures that the medication regimen is followed as prescribed, which is vital for the consumer's health.
What should I do if a medication is refused?
If a medication is refused, you should mark the corresponding box with an "R" on the record sheet. It's also important to document the reason for refusal in the consumer's notes or records to ensure that the healthcare team is aware of the situation.
Can I use the Medication Administration Record Sheet for multiple consumers?
No, each consumer should have their own Medication Administration Record Sheet. This helps maintain clear and accurate records for each individual, which is essential for effective medication management.
What should I do if I make a mistake on the form?
If you make a mistake while filling out the form, do not erase it. Instead, draw a line through the error and initial it. Then, write the correct information next to it. This keeps a clear record of what happened and maintains the integrity of the documentation.
How often should the Medication Administration Record Sheet be reviewed?
The Medication Administration Record Sheet should be reviewed regularly, ideally daily. This ensures that all medications are being administered as scheduled and allows for timely adjustments if any issues arise.
File Information
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record Sheet is used to document the administration of medications to consumers, ensuring accurate tracking of dosages and times. |
| Consumer Information | The form requires essential consumer information, including the consumer's name and the attending physician's name, to ensure proper identification and accountability. |
| Medication Tracking | Each hour of the day is represented on the form, allowing staff to record medication administration and any refusals or changes in medication status. |
| State Regulations | In many states, the use of a Medication Administration Record is governed by health care regulations. For example, in California, Title 22, Section 80064 outlines the requirements for medication administration documentation. |
| Recording Instructions | Staff are instructed to record medication administration at the time it occurs, ensuring real-time documentation and reducing the risk of errors. |
Common mistakes
Filling out a Medication Administration Record Sheet is a crucial task that requires attention to detail. However, many individuals make common mistakes that can lead to serious consequences. One frequent error is neglecting to include the consumer's name at the top of the form. Without this essential information, it becomes challenging to ensure that the correct medication is administered to the right person.
Another mistake involves failing to document the attending physician's name. This detail is vital for tracking the medication prescribed and for any potential follow-up questions that may arise. Omitting this information can create confusion and hinder effective communication among healthcare providers.
Many people also overlook the importance of accurately recording the date. The month and year should be clearly indicated, as this helps in maintaining an organized record over time. An incorrect date can lead to mismanagement of medication schedules, which can be detrimental to the consumer's health.
It’s not uncommon for individuals to skip filling in the hour when the medication is administered. Each medication has specific timing that must be adhered to for optimal effectiveness. Failing to record the correct hour can result in missed doses or overdoses, both of which pose significant risks.
Another frequent oversight is neglecting to mark the appropriate codes for medication status. For instance, if a medication is refused, it should be clearly noted with an “R”. Similarly, if a medication is discontinued, the “D” should be marked. Not recording these statuses can lead to misunderstandings about the consumer's treatment plan.
Additionally, some individuals forget to record at the time of administration. This can lead to inaccuracies in the record, making it difficult to track when medications were given. It’s essential to document each administration immediately to maintain an accurate timeline.
Another common error is not reviewing the form for completeness before submission. It’s easy to overlook small details, but a thorough check can prevent errors that might affect patient care. Taking a moment to ensure everything is filled out correctly can save a lot of trouble later on.
Finally, many people fail to keep a copy of the completed Medication Administration Record Sheet. Retaining a copy is essential for reference and for ensuring that all parties involved in the consumer's care are on the same page. This practice can help prevent miscommunication and ensure continuity of care.
Popular PDF Forms
Employer's Quarterly Federal Tax Return - Accurate hiring practices are crucial, as even temporary workers must be reported on Form 941.
To facilitate a smooth transaction, it is essential to utilize accurate documentation, and the PDF Templates for the Texas Real Estate Purchase Agreement form provide a reliable means to ensure all necessary terms are documented clearly and comprehensively.
Dl44 Pdf - The form includes a question about past applications in different names or numbers.